
- About Us
- Information
-

The Author ensures that the research has been conducted responsibly and ethically with adherence to all relevant regulations. read more..
- For Authors
- For Reviewer
- Manuscript Guidelines
- Membership
- Publication Ethics
-
- Journals
- Reprints
- e-Books
- Videos
- Policies
- Contact Us
 COVID-19
COVID-19
- Submissions



Full Text
Associative Journal of Health Sciences
Assessment of the Prognosis of Chronic Kidney Disease in People Living with HIV, Co-Morbid Hypertension and Diabetes Mellitus in Two Clinics in Maseru
Polile Paul Rasemoko1*, Mbongeni Adontsi2, Rantheba Itumeleng2 and Mokonyana Mohale2
1 M.Sc. in Pharmacology (NWU), National University of Lesotho, Faculty of Health Sciences, Lesotho
2 B, Pharm (Hons), National University of Lesotho, Faculty of Health Sciences, Lesotho
*Corresponding author:Mr. Rasemoko P. Polile, M.Sc. in Pharmacology (NWU), National University of Lesotho, Faculty of Health Sciences, Lesotho
Submission: March 18, 2026;Published: April 10, 2026

ISSN:2690-9707 Volume4 Issue4
Abstract
Background: Chronic kidney disease (CKD) has recently posed a significant public health concern in
lower-middle-income countries, including Lesotho. Despite comorbidities such as diabetes mellitus (DM),
hypertension (HTN), and Human Immunodeficiency Virus (HIV) worsening the condition, the combined
impact on Chronic kidney disease prognosis is not well understood in Lesotho.
Objective: The study aimed to assess the prognosis of chronic kidney disease in individuals living with
Human Immunodeficiency Virus, co-morbid hypertension, and diabetes mellitus, in two clinics in Maseru.
Method: This retrospective cross-sectional study was conducted at the Lesotho Defence Force (LDF)
and Domiciliary clinics using medical records in adult patients living with HIV, comorbid hypertension
and/or diabetes mellitus. The data was analysed with IBM SPSS version 20. The descriptive data were
presented as frequencies and percentages, while the continuous data were presented as means and
standard deviations.
Results: At the LDF clinic, 53.1% of the patients were female, and 46.9% were male. Patients living with
HIV were diagnosed with CKD stage 2, those with HIV and HTN had CKD stage 3a, and those with HIV,
HTN, and DM had CKD stage 3b. At the Domiciliary clinic, 56.7% of the were female, and 43.1% (56) were
male. Patients with HIV and HTN had CKD 2, and CKD 3a for patients with all three comorbidities.
Conclusion: Both CKD-EPI and MDRD methods showed minimal differences in eGFR. The CKD-EPI
formula in HIV-comorbid hypertensive and/or diabetic patients defines stage 3 renal failure earlier. HIV,
HTN, and DM were the major risk factors for poor CKD prognosis, often leading to kidney failure.
Keywords: Comorbidity; Prognosis; Chronic Kidney Disease; CKD-EPI; MDRD
Introduction
Chronic kidney disease (CKD) is the abnormality of kidney structure or function (defined by markers of kidney injury or decreased GFR) present for more than three months with health implications [1]. Kidneys can get damaged in several ways, often through physical injury or diseases like diabetes mellitus (DM) and hypertension (HTN). This is usually associated with a reduction in glomerular filtration rate (GFR) [2]. CKD has been recognised as a leading public health problem worldwide [3]. The global estimated prevalence of CKD is 13.4% [4], with a prevalence of 36.1% amongst those living with HIV and other comorbidities [5]. The burden of CKD is rising worldwide, with the fastest growth occurring in low-income countries like Lesotho [6]. In addition to poorly controlled DM and HTN, human immunodeficiency virus (HIV) plays an essential role in the epidemiology of CKD [7].
Chronic kidney disease due to DM and HTN affects nearly 5-7% of the world population [8]. The Modification of Diet in Renal Disease (MDRD) and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations are two commonly used equations for estimating GFR to evaluate the severity of CKD [9]. The MDRD equation estimates GFR using variables like serum creatinine, age, gender and race. The CKD-EPI equation was developed as an improvement over the MDRD equation [9]. It is aimed to provide more accurate estimates of GFR, especially in patients with higher GFR levels and across diverse populations [9].
Chronic Kidney Disease is the healthcare burden in Lesotho, and this results in patients’ morbidity, mortality and increased healthcare costs [6]. Primary healthcare facilities in Lesotho, including the major ones in Maseru, assess or manage hypertension (HTN), diabetes mellitus (DM), and HIV; however, none of these primary healthcare facilities screen for chronic kidney disease (CKD) progression. To date, the progression of CKD and its staging remains unknown. The number of patients living with CKD, HIV, co-morbid HTN and DM seems to be increasing [6]. These comorbidities independently are proven to increase the development and progression of chronic kidney disease, but the interaction between all these conditions on the prognosis of CKD remains poorly understood.
Evidence suggests that the increasing prevalence of CKD, which progresses to kidney failure (KF), increases healthcare resource utilisation [10]. CKD co-morbid HIV leads to a low quality of life in affected individuals with limited and reduced ability to perform their daily duties [11]. Understanding the prognosis of CKD in individuals with these comorbidities is essential due to the potential for a significant disease burden and healthcare impact. Improved understanding of CKD prognosis in this specific patient population can inform healthcare policies and resource allocation.
Materials and Methods
This study was a retrospective cross-sectional study which was conducted among outpatients living with HIV, comorbid hypertension and DM who had attended Lesotho Defence Force (LDF) and Domiciliary clinics. These two clinics are the major primary healthcare facilities in Maseru, which manage major risk factors to CKD, including HTN, DM and HIV, whilst keeping the laboratory results for HIV patients. The study population in two health facilities include people living with HIV alone and/ or comorbid HTN and DM who attend services in these clinics between January 1st 2022, and April 30th 2024. All files for men and women 18 years and older who had either HIV alone, HIV comorbid HTN and/or DM with at least two measurements of biomarkers (i.e. serum creatinine and BUN) were included in the study. The data collection tool recorded the average of the two most recent serum creatinine and BUN values. Incomplete files without serum creatinine and patient files before 1st January 2022 were excluded from the study.
The quantitative data were collected using a structured questionnaire adapted from similar studies comparing the estimated glomerular filtration rate based on the Modified Diet in Renal Disease (MDRD) and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formulas [8-10]. These ensure that all the validated questionnaires and methodologies used to measure the study’s objectives were valid and reliable.
The data was collected using a validated survey questionnaire adapted from similar studies [12-15] and modified to achieve the objectives of the current study. The information extracted from the patient’s files includes the patient demographic information (such as age, gender, body mass index), laboratory biomarkers, including creatinine, urea and Blood urea nitrogen (BUN) and serum creatinine was used to calculate the eGFR based on the Modified Diet in Renal Disease (MDRD) and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formulas, which were used to classify the patient’s CKD staging.
The study was approved by the National University of Lesotho International Review Board (NUL-IRB) and the Ministry of Health Research Ethics Committee (MOH-REC) (ID 58-2024). Confidentiality was ensured throughout the study. For anonymity and confidentiality, the patients were allocated serial numbers linking them to the files for record keeping.
Data was entered into a Microsoft Excel spreadsheet and analysed with the IBM SPSS statistical package (version 20). The patient’s data was captured on Microsoft 365 Excel®, and the patient’s demographic data, which included categorical variables, was analysed with descriptive statistics and presented as frequency and percentage per total, while the continuous variables were presented as a mean ± standard deviation (SD). The data were subjected to the Shapiro-Wilk test for normality. The chi-square was performed to assess the relationship between the independent categorical data, whereas Spearman’s correlation (non-parametric bivariate test) was performed to assess the factors that can influence the eGFR. The baseline male and female eGFR were calculated using CKD-EPI and MDRD equations as below.
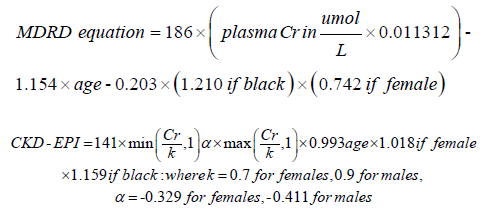
Where plasma Cr = plasma creatinine (umol/l)3.
Results
A total of 212 medical records were analysed, comprising 82 from the LDF clinic and 130 from the Domiciliary clinic. Among LDF records, 43.9% (n = 36) were females, and 56.1% (n=46) were males. In the Domiciliary Clinic, 56.9% (n=74) were females, while 43.1% (n=56) were males. The median age was 45.00 years [interquartile range (IQR) 35.00-52.00] at the LDF clinic, whereas at the Domiciliary clinic, the median 41.50 [interquartile range (IQR) 33.75-50.50]. At the LDF clinic, 48.3% (n= 38) had HIV only, 25.6% (n=21) had both HIV and HTN, whereas 28.0% (n=23) had HIV, HTN and DM (p=0.062). At Domiciliary, 60.0% (n=78) had HIV, 33.8% (n=44) had HTN and HIV, while the ones with HIV, HTN and DM were 6.2% (n=8), (p=0.933) (Table 1). The mean BMI for patients were (29.47 ± 4.00kg/m2, p=0.077) at the LDF clinic and (26.03±6.39kg/m2, p=0.115) at the Domiciliary clinic (Table 1). At the LDF clinic, the baseline average mean serum creatinine was 130.56±22.69umol/l, results were independent of age (p=0.055), whereas at the Domiciliary clinic, the baseline average mean serum creatinine was 84.09±27.67umol/l, and results significantly depend on age (p=0.011) (Table 1). The baseline average mean eGFR based on CKD-EPI was 54.96±13.59ml/min/1.73m2, and results significantly depend on age p<0.000), whereas for MDRD the baseline average mean was 47.92±11.15ml/min/1.73m2 (p=0.104) (Table 1). At the Domiciliary clinic, the baseline average mean eGFR based on CKD-EPI was 91.95±22.63ml/min/1.73m2 and results significantly depend on age p=0.025), whereas for MDRD the baseline average mean was 97.62±26.66ml/min/1.73m2 (p=0.045) (Table 1).
Table 1:Demographic and clinical characteristics of 212 HIV positive patients at LDF and Domiciliary clinics receiving ART treatment between January 2022 and April 2024. HTN -Hypertension; HIV-Human Imunodeficiency Virus; DM-Diabetes Mellitus; eGFR-estimated glomerular filtration rate; CKD-EPI-Chronic Kidney Disease Epidemiology Collaboration; MDRD- Modification of Diet in Renal Disease; BMI-Body mass index; BUN-Blood urea nitrogen m- Meters; m2-Meters squared Kg-Kilogram; mg/l-Milligrams per litre;umol/l-micromoles per litre; ARVs -Antiretrovirals; TDF/3TC/DTG-Tenofovir/lamivudine/Doltugravir; TDF/3TC/ EFV Tenofovir/lamivudine/Efavirenz; LPVr/AZT/EFV-Lopinavir/zudovudine/Efavirenz; ACEIs- Angitensing converting enzyme inhibitors; ARBs-Angiotenisin receptor blockers BB-Beta blockers; CCBs-Calcium channel blockers.

Our results showed that all HIV positive (n=82, 100%) patients at LDF were placed on TDF/3TC/DTG-based regimen, whereas 85.4% (n=111) of the patients at the Domiciliary clinic were placed TDF/3TC/DTG-based regimen, and 13.8% (n=18) of the patients at Domiciliary clinic were placed on TDF/3TC/EFV based regimen (Table 1). As shown in Table 1, the diuretics were the most used antihypertensives for the treatment of HTN in patients at the LDF clinic (n= 44, 53.7%) versus HTN patients’ Domiciliary clinic (n=49, 37.7%). The biguanides were mostly used in the management of DM among patients at the LDF clinic (n=23, 28.0%) versus a few (n=8, 6.2%) of the patients at the Domiciliary clinic (Table 1).
According to Table 2 below, when using CKD-EPI to compute eGFR, none of the patients had eGFR values ≥90ml/min/1.73m2 at LDF, whereas at Domiciliary, 60.7% (n=79) had eGFR values ≥90ml/min/1.73m2 which correspond to stage 1. Based on the CKD-EPI, 40.2% (n=33) of the patients at the LDF clinic and 30.8% (n=40) of the patients at the Domiciliary clinic had eGFR values 60- 89ml/min/1.73m2, which corresponds to CKD stage 2 (Table 2). As seen in Table 2, based on CKD-EPI, 28.1% (n=23) of patients at LDF and 4.6%(n=6) of the patients at Domiciliary had eGFR values 45-59ml/min/1.73m2, which correspond to stage 3a. Based on the CKD-EPI, 30.5% (n=25) of the patients at the LDF clinic and 2.3% (n=3) of the patients at the Domiciliary clinic had eGFR values, 30- 44ml/min/1.73m2, which correspond to stage 3b (Table 2). As seen in Table 2, using CKD-EPI, 1.22% (n=1) of the patients at LDF and 1.5 % (n=2) of the patients at Domiciliary clinic had eGFR values, 15-29ml/min/1.73m2, which correspond to stage 4. When using the MDRD, 63.8% (n=83) of the patients at Domiciliary had eGFR values greater than or equal to 90ml/min/1.73m2 (Table 2). As seen in Table 2, the number of patients who had eGFR values 60-89ml/ min/1.73m2 was twice at the Domiciliary clinic (n=36, 27.7%) versus the number of patients (n=15, 18.3%) at the LDF clinic. The majority (n=35, 42.7%) of the patients at LDF had eGFR ml/ min/1.73m2 is 6.2% compared to a few (n=8, 6.2%) of the patients at the Domiciliary clinic (Table 2). The majority (n= 29, 35.4%) of the patients LDF clinic had eGFR values 30-44ml/min/1.73m2 compared to a few (n=2, 1.5%) (Table 2).
Table 2:Comparisons of Clinical CKD staging based on CKD-EPI and MDRD eGFR in Patients at LDF (N=82) and Domiciliary clinics (N=130).

As shown in Table 3, looking in female patients at LDF clinic, the Spearman’s correlation shows a significantly negative correlation between age (r=-0.837, p<0.000), weight (r=-0.834, p<0.000), BMI (r= -0.760, p<0.000) and creatinine (r=-0.964, p<0.000) versus eGFR determined with the CKD-EPI formula. Our results demonstrated a significant negative correlation between age (r=-0.820, p<0.000), weight (r=-0.836, p<0.000), BMI (r=- 0.780, p<0.000) and creatinine (r=-0.979, p<0.000) versus eGFR determined with the MDRD formula. According to the male patients at LDF clinic, our results demonstrated a significant negative correlation between age (r=-0.828, p<0.000), weight (r=- 0.600, p<0.000), BMI (r=-0.634, p<0.000) and creatinine (r=-0.893, p<0.000) versus eGFR determined with the CKD-EPI formula (Table 3). Our results demonstrated a significant negative correlation between age (r=-0.813, p<0.000), weight (r=-0.611, p<0.000), BMI (r=-0.642, p<0.000) and creatinine (r=-0.895, p<0.000) versus eGFR determined with the MDRD formula (Table 3).
In the Domiciliary clinic, according to the female patients, the Spearman’s correlation shows a significantly negative correlation between age (r=-0.647, p<0.000), and creatinine (r=-0.948, p<0.000) versus eGFR determined with the CKD-EPI formula (Table 3). Our results demonstrated a significant negative correlation between age (r=-0.556, p<0.000) and creatinine (r=-0.974, p<0.000) compared to eGFR determined using the MDRD formula (Table 3). According to the male patients, the Spearman’s correlation shows a significantly negative correlation between age (r=-0.465, p<0.000), weight (r=-0.343, p=0.010) and creatinine (r=-0.913, p<0.000) versus eGFR determined with the CKD-EPI formula (Table 3). Our results demonstrated a significant negative correlation between age (r=-0.343, p=0.010), weight (r=-0.324, p=0.015) and creatinine (r=-0.973, p<0.000) versus eGFR determined with the MDRD formula (Table 3).
Table 3:Shows the Spearman’s correlation (bivariate analysis) of CKD-EPI and MDRD eGFR based on age, weight, BMI and creatinine in HIV co-morbid HTN and DM patients at LDF and Domiciliary clinics. N= number of participants; r= Correlation Coefficient; CKD-EPI-Chronic Kidney Disease Epidemiology Collaboration; MDRD- Modification of Diet in Renal Disease

Discussion
The study revealed that in Lesotho, the prevalence of CKD is higher in women compared to men. In 2016, a meta-analysis of 51 studies reporting sex-specific CKD prevalence found a mean prevalence of CKD of 14.6% in females and 12.8% in males, corresponding to a female: male prevalence ratio of 1.14 [16]. More recently, the 2017 Global Burden of Disease (GBD) study reported that the global age-standardised prevalence of CKD was 1.29 times higher in females than in males. It is generally accepted that, for any given age, the prevalence of milder forms of CKD (KIDGO Stage 1-3) is higher in females, while the opposite is true for kidney failure (KIDGO Stage 5) [16]. A recent review on the role of sex and gender in CKD have highlighted a complex interplay of biological, behavioural, cultural and socio-economic factors that may contribute to observed disparities [17].
Although TDF is implicated in causing nephrotoxicity, the likelihood of CKD progression is minimal due to monotherapy as compared to polypharmacy exhibited in other comorbidities. Similar to our results, one study revealed that people taking more than 3 drugs, which are predominantly excreted by the kidneys, have a heightened likelihood of developing CKD later in life, regardless of the diseases being treated, than those taking a single drug [18].
The equations for estimating GFR include plasma creatinine concentration, which is endogenously produced from skeletal muscle. For this reason, females who have less muscle mass than males would have lower plasma creatinine concentrations and consequently lower eGFR, which our study demonstrated [19].
Studies comparing the CKD-EPI equation with MDRD indicate that CKD-EPI yields more accurate results in estimating GFR and recommend the use of this equation in clinical practice 20. Although both formulas were mainly developed in patients with CKD, different population data were also taken into account in the CKD-EPI equation [20]. Matsushita et al. compared creatinine clearance, MDRD, and CKD-EPI formulas in one of their studies [20]. When the cases were analysed according to gender, there was a significant difference between GFR values in women. Whereas there was a statistically significant difference between creatinine clearance and MDRD, there was no significant difference between CKD-EPI with creatinine clearance [21].
The prevalence of CKD is 11.5% among individuals 70 years old with stage III and above CKD in Lesotho [6]. The increasing incidence of diseases, such as hypertension, obesity, and DM, constitutes a risk for CKD in our country and makes the early diagnosis and follow-up of CKD more important 6. The increase in the elderly population in our country and the decrease in renal function with ageing are indicators of an increase in the prevalence of CKD in the coming years.
For this reason, we believe that we have shown the importance of calculating GFR to make a more accurate assessment since creatinine values alone in the early diagnosis and management of CKD in elderly patients are not enough. Furthermore, the study showed that at the LDF clinic, the average eGFR using CKD-EPI for patients with HIV only is 66.53±8.02ml/min/1.73m2, while the average eGFR using CKD-EPI of patients living with HIV and HTN is 47.10±6.89ml/min/1.73m2 and that of patients living with HIV, HTN and DM is 43.04±9.53ml/min/1.73m2. These eGFR values calculated using CKD-EPI correspond to stage 2, stage 3a and stage 3b, respectively, in these patient populations. On the other hand, the average eGFR using MDRD for patients living with HIV only is 57.17±6.80ml/min/1.73m2, while for people living with HIV and HTN is 41.40±5.98ml/min/1.73m2 and for those living with HIV, HTN and DM is 39.36±9.03ml/min/1.73m2. These eGFR values obtained using MDRD correspond to stage 3a for people living with HIV only, 3b for HIV and HTN and also 3b for those living with HIV, HTN and DM. This shows a slight difference between CKD-EPI and MDRD.
The study also revealed the importance of taking baseline creatinine levels when patients are introduced to ART. This is of paramount importance in monitoring CKD and ultimately results in a better prognosis [22]. Again, it was noted that the majority of patients were obese and overweight; therefore, it is crucial to highlight the importance of weight management in this patient population. Patients should be mindful of their diet and ensure at least 30 minutes of regular exercise of any kind. The bivariate analysis demonstrated a statistically significant negative correlation between age, weight, body mass index and creatinine versus eGFR determined with both CKD-EPI and MDRD. Both formulas incorporate age and creatinine, which are inversely proportional to the estimated glomerular filtration rate.
The research team acknowledge the following limitations, which may have affected the findings and interpretations: Two facilities were assessed, and the conclusions made cannot be generalized to give the overall CKD in Lesotho primary health facilities. Additionally, incomplete data had to be excluded in the analysis, which reduced the sample size, and may have affected the conclusiveness of the data and was therefore taken into consideration.
Conclusion
HIV, HTN and DM are major risk factors for the prognosis of CKD in two healthcare facilities in Maseru. The majority of the patients with these comorbidities were diagnosed with CKD stage 3. Early detection of CKD and proper management of these comorbidities may decrease the progression to kidney failure. MDRD and CKD-EPI equations can significantly be employed in the determination of the patients at risk of CKD in HIV patients with other comorbidities at affordable cost.
Acknowledgement
The authors would also like to thank the NUL-IRB and MOHREC for granting ethics approval for conducting this study and the health facilities for their cooperation during data collection.
Declarations
Funding
The study was partially funded by the Lesotho National Manpower Development Secretariat (NMDS) as student project fee. Other costs of the study was self-funded by the authors.
Competing interests
All authors declare no conflict of interest.
Ethical approval
Approval by the National University of Lesotho International Review Board (NUL-IRB) and Ministry of Health Research Ethics Committee (MOH-REC) (ID 58-2024). The authors obtained consent to publish from the MOH of Lesotho and two clinics.
Declaration of patients consent
The informed consent waiver was obtained in the present study since the study used secondary data and was retrospective.
Use of Artificial Intelligence (AI)
Assisted Technology for Manuscript Preparation: The author (s) confirm that the Zotero reference manager, grammer checker were the only used AT tools during the manuscripts. However, none of the Assisted Technology were used for writing the manuscripts and no images were manipulated with the application of AI.
References
- Damtie S, Biadgo B, Baynes HW, Ambachew S, Melak T, et al. (2018) Chronic kidney disease and associated risk factors assessment among diabetes mellitus patients at a tertiary hospital, Northwest Ethiopia. Ethiopian Journal of Health Sciences 28(6): 691-700.
- Barsoum RS (2006) Chronic kidney disease in the developing world. New England Journal of Medicine 354(10): 997-999.
- Bello AK, Alrukhaimi M, Ashuntantang GE, Basnet S, Rotter RC, et al. (2017) Complications of chronic kidney disease: Current state, knowledge gaps, and strategy for action. Kidney International Supplements 7(2):122-129.
- Hill NR, Fatoba ST, Oke JL, Hirst JA, O’Callaghan CA, et al. (2016) Global prevalence of chronic kidney disease - A systematic review and meta-analysis. PLoS One 11(7): e0158765.
- Ene-Iordache B, Perico N, Bikbov B, Carminati S, Remuzzi A, et al. (2016) Chronic kidney disease and cardiovascular risk in six regions of the world (ISN-KDDC): A cross-sectional study. The Lancet Global Health 4(5): e307-319.
- Chitja M, Malope S, McGuire C, Steer-Massaro RN, Killilea O, et al. (2021) A report of the first year of dialaysis treatment availability in the mountain kingdom of Lesotho. Le Med J 15(1): 17-24.
- Coresh J (2017) Update on the Burden of CKD. Journal of the American Society of Nephrology 28(4): 1020-1022.
- Couser WG, Remuzzi G, Mendis S, Tonelli M (2011) The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney International 80(12): 1258-1270.
- Levey AS, Stevens LA, Schmid CH, Zhang Y, Castro AF, et al. (2009) A new equation to estimate glomerular filtration rate. Annals of Internal Medicine 150(9): 604.
- Ekrikpo UE, Kengne AP, Bello AK, Effa EE, Noubiap JJ, et al. (2018) Chronic kidney disease in the global adult HIV-infected population: A systematic review and meta-analysis. PLoS One 13(4): e0195443.
- Levin A, Tonelli M, Bonventre J, Coresh J, Donner JA, et al. (2017) Global kidney health 2017 and beyond: A roadmap for closing gaps in care, research, and policy. The Lancet 390(10105): 1888-1917.
- Ahmed S, Jafri L, Khan AH (2017) Evaluation of “CKD-EPI Pakistan” Equation for estimated glomerular filtration rate (eGFR): A comparison of eGFR prediction equations in Pakistani population. Journal of the College of Physicians and Surgeons Pak 27(7): 414-418.
- Cepni AI, Basat SU, Pala E (2018) Comparison of MDRD and CKD-EPI formulas for estimating glomerular filtration rate in elderly preoperative patients. Journal of Academic Research in Medicine 8: 9-14.
- Fontela PC, Winkelmann ER, Ott JN, Uggeri DP (2014) Estimated glomerular filtration rate in patients with type 2 diabetes mellitus. Rev Assoc Med Bras 60(6): 531-537.
- Korhonen PE, Kivelä SL, Aarnio PT, Kautiainen H, Järvenpää S, Kantola IM (2011) Estimating glomerular filtration rate in hypertensive subjects: Comparison of the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) and Modification of Diet in Renal Disease (MDRD) study equations. Annals of Medicine 44(5): 487-493.
- Bikbov B, Perico N, Remuzzi G (2018) Disparities in chronic kidney disease prevalence among males and females in 195 countries: Analysis of the Global Burden of Disease 2016 Study. Nephron 139(4): 313-318.
- Carrero JJ, Hecking M, Chesnaye NC, Jager KJ (2018) Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nature Reviews Nephrology 14(3): 151-164.
- American Diabetes Association (2014) Diagnosis and classification of diabetes mellitus. Diabetes Care 37(Supplement_1): S81-90.
- Habas E, Habas E, Khan FY, Rayani A, Habas A, et al. (2022) Blood pressure and chronic kidney disease progression: An updated review. Cureus 14(4): e24244.
- Matsushita K, Mahmoodi BK, Woodward M, Emberson JR, Jafar TH, et al. (2012) Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA 307(18): 1941-1951.
- Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, et al. (2015) Worldwide access to treatment for end-stage kidney disease: A systematic review. The Lancet 385(9981): 1975-1982.
- Levin A, Hemmelgarn B, Culleton B, Tobe S, McFarlane P, et al. (2008) Guidelines for the management of chronic kidney disease. Canadian Medical Association Journal 179(11): 1154-1162.
© 2026 Polile Paul Rasemoko. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and build upon your work non-commercially.
Editor In Chief







.jpg)

























Signup for Newsletter

Quick Links
 Editorial Board Registrations
Editorial Board Registrations Submit your Article
Submit your Article Refer a Friend
Refer a Friend Advertise With Us
Advertise With UsOur Recent Edition

.jpg)



Top Editors




.jpg)

















.bmp)
.jpg)
.png)
.jpg)













.jpg)






.png)

.png)




.png)




Financial Support

Sponsors

Latest e-Books

Latest Video

 a Creative Commons Attribution 4.0 International License. Based on a work at www.crimsonpublishers.com.
Best viewed in
a Creative Commons Attribution 4.0 International License. Based on a work at www.crimsonpublishers.com.
Best viewed in