
- About Us
- Information
-

The Author ensures that the research has been conducted responsibly and ethically with adherence to all relevant regulations. read more..
- For Authors
- For Reviewer
- Manuscript Guidelines
- Membership
- Publication Ethics
-
- Journals
- Reprints
- e-Books
- Videos
- Policies
- Contact Us
 COVID-19
COVID-19
- Submissions



Full Text
Research in Medical & Engineering Sciences
Is It Effective For Acupuncture In Treating Postoperative Ileus? ---- A Systematic Review and Meta-Analysis
Jian Wang1, Wei Tang1, Jun Guo1, Wen-ting Chen1, Gui-jie Yu1, Rui Feng1, Lan Yuan1, Guo-qiang Fu1 and Yue Yong2, Jian-gang Song1*
1Department of Anesthesiology, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, China
2Research institute of Acupuncture and anesthesia, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, China
*Corresponding author: Jian-gang Song, Department of Anesthesiology, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, China
Submission: August 22, 2020Published: October 27, 2020

ISSN: 2576-8816Volume9 Issue1
Abstract
Background:Acupuncture may promote early recovery of postoperative ileus (POI). This meta-analysis aimed to determine the efficacy of acupuncture on outcomes after elective surgery.
Material and Methods: We searched database of PUBMED, EMBASE, the Cochrane Central Register of Controlled Trials from their inception to Aug. 2019, and selection criteria is randomized controlled trials (RCT). Primary outcome was time to first passage of flatus(d). Secondary outcomes included time to tolerated solid food(d), time to first bowel movement(d), time of first defecation(d), duration of hospital stay(d).
Result: We identified 9 studies that recruited 910 participants for inclusion in our review. Compared with other non-pharmacy treatments, acupuncture treatment yielded an improved on mean time to first passage of flatus in postoperative patients (MD=-0.67; 95% CI, [-1.33, -0.01], p= 0.000; I2= 94.7%), a shorten time to tolerated solid food (MD=-0.33; 95% CI, [-0.62, -0.04], p= 0.320; I2`=14.5%), an earlier recovery of bowel movement (MD=-0.43; 95% CI, [-0.74, -0.11], p= 0.004; I2= 73.9%), an improved on mean time of first defecation (MD=-1.33; 95% CI, [-1.90, -0.76], p= 0.000, I2= 83.2%), and reduced hospital stay (MD=-0.43; 95% CI, [-0.68, -0.19], p=0.049, I2=52.6%),
Conclusion: This review identified the evidence of acupuncture for postoperative patients in improving recovery of gastrointestinal function. This benefit of acupuncture should be a potential non-pharmacotherapy in the management of postoperative ileus.
Keywords: Postoperative ileus; Meta-analysis; Acupuncture; Systematic review
Introduction
Postoperative ileus (POI) is a transient cessation of coordinated propulsive motility following abdominal surgery. The clinical manifestations include abdominal pain, distension, nausea and vomiting, stop passing stools of flatus, or unable to tolerate a solid diet. Postoperative ileus is a transient process, but if this process prolonged, complications such as wound dehiscence, intestinal anastomotic fistula, intra-abdominal infection, intestine ischemia, and aspiration pneumonia may occur [1-3]. Postoperative ileus is a significant predictor of extended hospital stays and postoperative costs in patients undergoing colectomy in the United States [4]. According to statistics, the United States cost more than $1.46 billion in the treatment of POI each year [5].
The treatment strategies of POI consist of perioperative an aesthetic and analgesic management, feeding soon after surgery, avoidance of nasogastric tube feeding, early ambulation, epidural analgesia, fluid restriction and minimally invasive surgery, etc., none of them has been successfully in preventing POI completely [6,7]. Acupuncture therapy is one of traditional Chinese medicine treatment, and its history is more than 3000 years [8]. Stimulation through the points, meridians, makes the treatment effective. Acupuncture combined with electrical stimulation is called electro-acupuncture, ear acupuncture is referred to puncturing the reaction spots of the auricle to treat diseases, and head needle is referred to puncturing the head and neck region as playing a role of treatment. A study reported by Ng SS suggests that electro-acupuncture reduced the duration of postoperative ileus compared with no acupuncture or sham acupuncture
treatment, after laparoscopic colorectal surgery [9]. However, a
later study reported that true acupuncture did not reduce POI more
significantly than sham acupuncture [10]. Past research showed
inconsistent results for acupuncture on postoperative ileus. Until
now, there was lack of effective evidence about the curative effect of
acupuncture in POI. Therefore, we carried out a systemic evaluation
and meta-analysis, on the basis of randomized controlled trials
research to evaluate whether acupuncture treatment could shorten
the time of postoperative ileus or not.
Methods
The main objective of this review was to examine whether acupuncture could reduce the time of postoperative ileus and promote recovery.
Criteria for considering studies in this review
Inclusion criteria included
Randomized controlled trials (RCTs).
A. Intra-peritoneal surgery patients.
B. Comparing acupuncture treatment or combined therapy with
electro-acupuncture with no treatment, sham acupuncture for
intraperitoneal surgery patients.
C. Full-text articles and detailed clinical data were available.
We included randomized controlled trials (RCTs) that
compared acupuncture with any other treatment for the treatment
of postoperative ileus among patients undergoing intraperitoneal
surgery. Trials with non-abdominal surgery were excluded.
Two investigators (GJ and TW) conducted literature retrieval
independently, according to the selection conditions, and reached
consensus on each citation.
Primary outcome
Time to first passage of flatus.
Secondary outcomes
Time to tolerated solid food, time to first bowel movement, time of first defecation, duration of hospital stay.
Searching strategy
Database of PUBMED, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL) were searched. There were no restrictions used during the search related to the publication year, publication language. The following search strategy was used in EMBASE and was modified accordingly for other databases:[(((‘intestine obstruction’ OR ‘postoperative complication’ OR (‘ileus’ OR ‘intestine pseudo obstruction’ OR ‘pseudo obstruction’ OR ‘pseudo-obstruction’ OR ‘pseudo obstruction’)) AND (‘acupuncture’ OR ‘acupuncture analgesia’ OR ‘electroacupuncture’ OR ‘acupuncture point’ OR ‘acupuncture therapy’ OR (‘acupuncture’ OR ‘acupoint’ OR ‘moxibustion’ OR ‘acupressure’ OR ‘auriculotherapy’ OR ‘auricular acupuncture’))) AND ((‘randomized controlled trial’ OR ‘randomization’ OR ‘controlled study’ OR ‘multicenter study’ OR ‘phase 3 clinical trial’ OR ‘phase 4 clinical trial’ OR ‘double blind procedure’ OR ‘single blind procedure’) NOT ((‘animal’ OR ‘nonhuman’:ab,ti) NOT (‘human’:ab,ti AND (‘animal’ OR ‘nonhuman’:ab,ti))))) AND (‘gastrointestinal’ OR ‘digestive system function disorder’)].
Data extraction and management
The quality assessment of the methodology was based on Cochrane Handbook for Systemic Reviews of Interventions 5.0.0 (Higgins 2008). “yes, no, unclear” represented a low risk of bias, a high risk of bias, and insufficient detail respectively in the study. The following items: “random sequence generation”, “allocation concealment”, “blinding of participants and personnel”, “blinding of outcome assessment”, “incomplete outcome data”, “selective reporting”, and “other bias” were assessed. Two researchers (GJ and TW) evaluated the eligible trials separately and finally reached a consensus Figure 1 & 2.
Figure 1: Study flow chart Data from 9 articles included in the meta-analysis.

Figure 2: Risk of bias assessment of included studies: Risk of bias graph (A), risk of bias summary (B). The cohrane “risk of bias” tool was used for quality assessment. Green for “yes”, red for “no” and yellow for “unclear”.

Statistical analysis
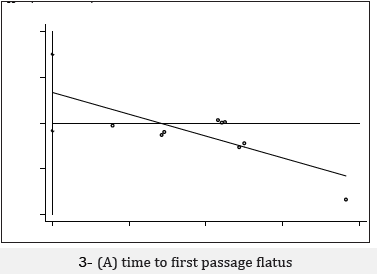
This meta-analysis was performed by using Review Manager 5.3 and STATA 14.0. Risk ratios and 95% confidence intervals (CIs) were calculated for dichotomous variables. Mean differences (MDs) and 95% CIs were calculated for continuous variables. Calculated pooled estimates of the mean differences in outcomes between groups by using a random-effects model. Sensitivity analyses was carried out before the comparation between groups. In order to assess the possibility of publication bias, we constructed a funnel plot (Figure 3). We are using Egger test to assess the asymmetry of funnel plot, a p value<0.1 regarded as a significant publication bias. We used the Q test and I2 testing to assess heterogeneity between studies. Studies with an I2 statistics ranging from 25% to 50%, indicated low heterogeneity, I2 statistics ranging from 50% to 75%, indicated moderate heterogeneity, and I2 statistics >75% was considered to have high heterogeneity. Greater than 50% of the I2 statistics represented significant heterogeneity in these studies11.
Figure 3: Meta-analyses of acupuncture on postoperative ileus: Outcomes assessed are:(A) time to first passage flatus, (B) time to tolerated solid food, (C) first bowel movement, (D) first defecation (E) hospital stay

Results
A total of 90 records were retrieved by searching various databases. 45 duplicate records were excluded, and 15 records were excluded after review of titles and abstracts. 24 studies were selected as being potentially eligible for inclusion into this systematic review. After reading the full-text articles, 9 RCTs (published between 2008 and 2019) including 910 participants were finally included [9,10]. The process of trial selection was shown in the study flow chart [11-18] (Figure 1).
Characteristics of Included studies
Table 1 shows the characteristics of included studies. Table 2 shows the outcome data of included studies. Figure 2 shows “risk of bias” assessment results. The seven included RCTs were published between 2008 and 2019. 2 trials compared acupuncture combined with traditional Chinese medicine to conventional treatment. 1 trial compared acupuncture against with sham acupuncture ,1 trial compared patients with sham acupuncture and no intervention, 6 trials compared acupuncture against with routine treatment or postoperative nursing. The sample size was ranging from 5 to 189 (449 cases in the treatment group received acupuncture / EA treatment and 461 cases in the control group. A total of 910 participants were included in the data synthesis.)
Table 1:Characteristics of included studies.

Table 2:Outcome data of included studies.

Quality assessment
Risk-of-bias assessment of the included studies is presented in Figure 2. The 9 included RCTs had a low risk of bias in randomized sequence generation and allocation concealment. In some of the selected studies, there was no detailed explanation on how to blind patients for acupuncture treatment [9,12,13] which suggested that might cause study bias.
Primary endpoint
Time to first passage flatus: In a pooled analysis of all 9 studies, the treatment of acupuncture led to a greater improvement for time to first passage flatus than other non-pharmacy treatments, with statistically significant between-study heterogeneity [Heterogeneity chi-squared = 151.86 (d.f. = 8), p= 0.000; I2= 94.7%; Figure 2.]. In this analysis, no publication bias was evident (P>|t|= 0.101, Figure 3a), however, further sensitivity analysis shows no substantial change in the effect size of the combined effect -0.67 (-1.33, -0.01).
Secondary endpoints
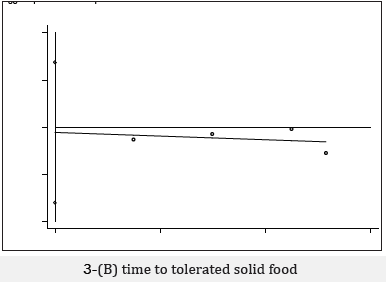
First tolerated solid food: Pooled analysis of the 4 studies that assessed time to tolerated solid food showed a higher likelihood of quickly recovery when patients treated with acupuncture compared with other treatment, with low between-study heterogeneity [ Heterogeneity chi-squared =3.51 (d.f. = 3), p= 0.320; I2`=14.5% Figure 2]. In this analysis no publication bias was evident (P>|t|=0.773, Figure 3b & 3c). sensitivity analysis shows no substantial change in the effect size of the combined effect was found -0.33(-0.62, -0.04)
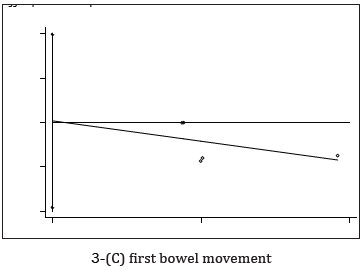
First bowel movement: Pooled analysis of the 5 studies that assessed time of first bowel movement showed a higher likelihood of quickly recovery when patients treated with acupuncture compared with other treatment, with statistically significant between-study heterogeneity [Heterogeneity chi-squared=15.31 (d.f. = 4), p= 0.004; I2= 73.9%, Figure 2]. In this analysis no publication bias was evident (P>|t|=0.955, Figure 3d). Sensitivity analysis shows no substantial change in the effect size of the combined effect was found -0.42(-0.74, -0.11)
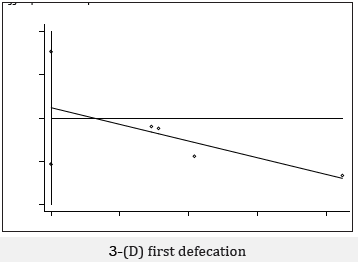
First defecation: Pooled analysis of the 4 studies that assessed time of first defecation showed a higher likelihood of quickly recovery when patients treated with acupuncture compared with other treatment, with statistically significant between-study heterogeneity [Heterogeneity chi-squared =17.84 (d.f. = 3), p= 0.000, I2= 83.2%, Figure 2]. In this analysis no publication bias was evident (P>|t|=0.515, Figure 3e). Sensitivity analysis shows no substantial change in the effect size of the combined effect was found -1.33(-1.90, -0.76)
Figure 4: Egger test of acupuncture on postoperative ileus: ,

Hospital stay
Pooled analysis of the 7 studies that assessed time of hospital stay showed a higher likelihood of quickly recovery when patients treated with acupuncture compared with other treatment, with moderate between-study heterogeneity [Heterogeneity chisquared =12.65 (d.f. = 6), p=0.049, I2=52.6%, Figure 2]. In this analysis no publication bias was evident (P>|t|=0.423, Figure 3f). Sensitivity analysis shows no substantial change in the effect size of the combined effect was found -0.43(-0.68, -0.19)
Discussion
In this meta-analysis, we identified 9 RCTs investigating the
effect of acupuncture on postoperative patients. Our result show
that, compared with non-pharmacy treatment, acupuncture
treatment can shorten the time to first passage flatus after
operation. Furthermore, compared with other control treatment,
acupuncture offers faster recovery time to tolerated solid food, first
bowel movement, first defecation and shorter hospital stay. Thus,
evidence seems to support that acupuncture improve postoperative
gastrointestinal motor function.
As two important indicators of bowel activity, the time of first
bowel movement and first passage of flatus have been widely used,
however, these indicators also have limitations, such as objective
measurement of motility and time consuming [19,20]. Various
clinical endpoints of POI have been used in studies regarding POI
diagnosis, but there is no consensus on which clinical parameter
is the best one for assessment of gastrointestinal (GI) transit
[6,21,22]. Recent years, new techniques have been used to assess the
function of gastrointestinal movements. For example, Sitz marker
has been used to evaluate postoperative recovery of small bowel
movement, by counting the number of remnants Sitz markers in
the small intestine that did not pass through ileocecal valve through
radiography [23]. The Smart Pill is another swallowable device
that record parameters within gastrointestinal tract, such as pH, temperature and intracavitary pressure, to analyze gastrointestinal
transit times and smooth muscle activity in vivo. Innovative devices
lead to a visualization or physical and chemical monitoring of the
complete GI tract. More and more objective parameters could be
provided to record and evaluate the duration and severity of POI,
which is conducive to improving the reliability of clinical research
[1,24].
Patients accepting acupuncture intervention had a significant
shortened hospital stay, data were extracted from five included
studies [12-16]. Hospital stay was affected by a number of factors,
in particular postoperative complications. Whether acupuncture
would affect postoperative complications for POI, better-quality
studies would be needed for future update. We didn’t combine and
analyze the data of postoperative complications in this study since
insufficient data was reported.
As shown in Figures 2 & 3. Robust and consistent findings
were produced by our study that suggest benefits of acupuncture
treatment on improving POI (time to first passage flatus, time
to tolerated solid food, first bowel movement, first defecation,
hospital stay). Not only that acupuncture has a similar effect has
been reported from several animal models and clinical studies
[9,14,25]. However, few researches have been contributing to new
insights into the mechanisms of acupuncture improving POI. The
hypothesis that acupuncture may help regulate the gastrointestinal
tract through the autonomic nervous system has been confirmed.
Several animal studies have shown that the effect of acupuncture
is mediated through parasympathetic efferent pathways [26,27]
especially, the effect of acupuncture on gastrointestinal function
might through the vagus nerve [25,28]. Acupuncture has been
used to treat functional gastrointestinal diseases and symptoms
in Asian countries for thousand years. It is being widely accepted
by clinicians and patients in the world today. Similarly, our study
revealed the clinical effects of acupuncture on improving POI,
further large sample experiment was suggested, and further
mechanism research should be carried out.
There are some limitations of this meta-analysis. First,
Insufficient quantity studies were included, some of published
studies in this review have a small sample size, which may
skew the results. We have retrieved acupuncture treatment of
postoperative ileus (database of PUBMED, EMBASE, and CENTRAL).
Unfortunately, there were a small quantity of RCTs or observational
studies, and most of them are not in line with inclusion criteria
of this study. further large sample experiment was suggested.
Second, the potential exists to cause bias. For example, publication
bias might exist because research with statistically significant
results is potentially more likely to be submitted and published
than work with null or non-significant results [29]. Third, various
acupuncture methodologies of the included studies also made bias
inevitable. The acupoints selection and treatment strategies used in
the included studies were much the same. Beyond that, there were
several factors influencing on the efficacy of acupuncture (moment
of treatment and time interval, acupuncture manipulation, patient’s age, somatotype, physical and functional status, etc.) [30]. Among
the included studies, Ng SS et al. [9] selected the elderly patients
to observe the postoperative GI function, which was different
from other studies on age. Age was found to be an independent
predictor for either prolonged ileus or duration of ileus [31].
Various acupoints selected during acupuncture treatment,
treatment sessions, duration and frequency of electric stimulation
might also contribute to the main cause of bias [32]. Homogeneity
of interventions should be handled carefully. High and moderate
heterogeneity was detected in this study on the comparison of
endpoints. Sensitivity analysis and subgroup analysis methods
were also used to deal with high heterogeneity. We used the random
effects model to justify the treatment effects in this meta-analysis
[33]. Notwithstanding its limitation, our findings can clearly
indicate the benefits of acupuncture in the clinical management of
postoperative ileus.
Conclusion
In summary, we conducted a meta-analysis of 9 RCTs to investigate the effect of acupuncture treatment in POI. This review identified the evidence of acupuncture for postoperative patients in improving recovery of gastrointestinal function. This benefit of acupuncture should be a potential non-pharmacotherapy in the management of postoperative ileus.
Acknowledgement
We thank Dr. Stanley Tao from Shanghai Ruihui Biotech for his valuable assistance in statistical analysis of this study.
Funding
The present study is supported by the project of the National Natural Science Foundation of China (No. 81703898).
References
- Petra GB, Fanny FB, Misha D, Kevin WY, Ignace HJ, et al. (2014) Reduction of postoperative ileus by early enteral nutrition in patients undergoing major rectal surgery: prospective, randomized, controlled trial. Ann Surg 259: 649-655.
- Melis M, Fichera A, Ferguson MK (2006) Bowel necrosis associated with early jejunal tube feeding: A complication of postoperative enteral nutrition. Arch Surg 141(7): 701-704.
- Gomes GF, Pisani JC, Macedo ED, Campos AC (2003) The nasogastric feeding tube as a risk factor for aspiration and aspiration pneumonia. Curr Opin Clin Nutr Metab Care 6(3): 327-333.
- Iyer S, Saunders WB, Stemkowski S (2009) Economic burden of postoperative ileus associated with colectomy in the United States. J Manag Care Pharm 15(6): 485-494.
- Goldstein JL (2007) Inpatient economic burden of postoperative ileus associated with abdominal surgery in the United States 32: 82-90.
- Van Bree SH, Andrea N, Cathy C, Pedro J, Gianluca M, et al. (2012) New therapeutic strategies for postoperative ileus. Nat Rev Gastroenterol Hepatol 9(11): 675-683.
- Barletta JF, Senagore AJ (2014) Reducing the burden of postoperative ileus: evaluating and implementing an evidence-based strategy. World J Surg 38(8): 1966-1977.
- Zhuang Y, Xing JJ, Li J, Zeng BY, Liang FR (2013) History of acupuncture research. Int Rev Neurobiol 111: 1-23.
- Ng SS (2013) Electroacupuncture reduces duration of postoperative ileus after laparoscopic surgery for colorectal cancer. Gastroenterology 144: 307‐313.
- Deng G, W Douglas, Jose G, Yi C, Theresa A, et al. (2013) A phase II, randomized, controlled trial of acupuncture for reduction of Postcolectomy Ileus. Annals of Surgical Oncology 20(4): 1164‐1169.
- Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414): 557-560.
- Meng ZQ, Kay M, Joseph S, Hui Ting P, Ying Q, et al. (2010) Electro-acupuncture to prevent prolonged postoperative ileus: a randomized clinical trial. World Journal of Gastroenterology 16(1): 104‐111.
- Garcia MK, John M, Miguel A, David Z, Barry W, et al. (2008) Acupuncture to prevent prolonged postoperative ileus: A randomized controlled trial. Medical Acupuncture 20(2): 83-88.
- Chae HD, Kwak MA, Kim IH (2016) Effect of acupuncture on reducing duration of postoperative ileus after gastrectomy in patients with gastric cancer: A pilot study using sitz marker. Journal of Alternative and Complementary Medicine 22(6): 465‐472.
- Jung SY, Chae HD, Kang UR, Kwak MA, Kim IH (2017) Effect of acupuncture on postoperative ileus after distal gastrectomy for gastric cancer. J Gastric Cancer 17(1): 11-20.
- Liu MY, Wang CW, Wu ZP, Li N (2017) Electroacupuncture for the prevention of postoperative gastrointestinal dysfunction in participants undergoing vascular laparotomy under general anesthesia: A randomized controlled rial. Chin Med 12: 5.
- You XM, Xin S, Liang M, Jian H, Hong G, et al. (2015) Randomized clinical trial comparing efficacy of simo decoction and acupuncture or chewing gum alone on postoperative ileus in patients with hepatocellular carcinoma after hepatectomy. Medicine 94(45): e1968.
- Yang Y, Hong Q, Zhao L, Yu Z, Xian W, et al. (2017) Comparison of efficacy of simo decoction and acupuncture or chewing gum alone on postoperative ileus in colorectal cancer resection: a randomized trial. Scientific Reports 19(7): 37826.
- Maffezzini M, Campodonico F, Canepa G, Gerbi G, Parodi D (2008) Current perioperative management of radical cystectomy with intestinal urinary reconstruction for muscle-invasive bladder cancer and reduction of the incidence of postoperative ileus. Surgical Oncology 17(1): 41-48.
- Bungard TJ, Kale P (2012) Prokinetic agents for the treatment of postoperative ileus in adults: a review of the literature. Pharmacotherapy 19(4): 416-423.
- Vather R, Trivedi S, Bissett I (2013) Defining postoperative ileus: Results of a systematic review and global survey. Journal of Gastrointestinal Surgery 17(5): 962-972.
- Wu Z, Boersema G, Dereci A, Menon A, Jeekel J, et al. (2015) Clinical endpoint, early detection, and differential diagnosis of postoperative ileus: a systematic review of the literature. European Surgical Research 54(3-4): 127-138.
- Sadik R, Stotzer P, Simrén M, Abrahamsson H (2008) Gastrointestinal transit abnormalities are frequently detected in patients with unexplained GI symptoms at a tertiary centre. Neurogastroenterology & Motility 20(3): 197-205.
- Vilz TO, Dimitrios P, Philipp L, Rolf F, Anke E, et al. (2016) SmartPill® as an objective parameter for determination of severity and duration of postoperative ileus: study protocol of a prospective, two-arm, open-label trial (the PIDuSA study). BMJ Open 8: 6(7): e011014.
- Fang, J, Jian q, Xiao m, Jun y, Yi L, et al. (2017) Electroacupuncture treatment partly promotes the recovery time of postoperative ileus by activating the vagus nerve but not regulating local inflammation. Scientific Reports 7: 39801.
- Wang JJ, Qin M, Xiao D, Yu X, Liang W, et al. (2007) Electro-acupuncture of Foot Yangming regulates gastric activity possibly through mediation of the dorsal vagal complex. American Journal of Chinese Medicine 35(3): 455-464.
- Torres RR, Ghassan Y, Geber P, Priya M, Maria d, et al. (2014) Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nat Med 20(3): 291-295.
- The FO, Cailotto C, Van J, Jonge W, Bennink J, et al. (2011) Central activation of the cholinergic anti-inflammatory pathway reduces surgical inflammation in experimental post-operative ileus. British Journal of Pharmacology 163(5): 1007-1016.
- Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR (1991) Publication bias in clinical research. Lancet 337(8746): 867-872.
- Zheng J, Chen B, Guo Y, Guo Y (2015) Analysis on the factors that cause the difference of acupoints synergy effect. Chinese Acupuncture & Moxibustion 35(7): 719-722.
- Svatek RS, Mark B, Michael BW, Surena F, Ashish M, et al. (2010) Age and body mass index are independent risk factors for the development of postoperative paralytic ileus after radical cystectomy. Urology 76(6): 1419-1424.
- Chapuis PH, Les B, Anil K, Matthew J, Peter S, et al. (2013) Risk factors for prolonged ileus after resection of colorectal cancer: an observational study of 2400 consecutive patients. Annals of Surgery 257(5): 909-915.
- Moreno SG, Alex J, John R, Ades AE, Keith R, Nicola J, et al. (2012) A generalized weighting regression-derived meta-analysis estimator robust to small-study effects and heterogeneity. Statistics in Medicine 31(14): 1407-1417.
© 2020 Jian-gang Song. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and build upon your work non-commercially.
Editor In Chief







.jpg)

























Signup for Newsletter

Quick Links
 Editorial Board Registrations
Editorial Board Registrations Submit your Article
Submit your Article Refer a Friend
Refer a Friend Advertise With Us
Advertise With UsOur Recent Edition

.jpg)



Top Editors




.jpg)

















.bmp)
.jpg)
.png)
.jpg)













.jpg)






.png)

.png)




.png)




Financial Support

Sponsors

Latest e-Books

Latest Video

 a Creative Commons Attribution 4.0 International License. Based on a work at www.crimsonpublishers.com.
Best viewed in
a Creative Commons Attribution 4.0 International License. Based on a work at www.crimsonpublishers.com.
Best viewed in